On Saturday, Oct. 21, 2023, Cardiometabolic Health Congress (CMHC) celebrated the final day of its 18th Annual Conference, Social Determinants and Digital Advances in Cardiorenal Metabolic Health. The educational sessions, held at the iconic Boston Park Plaza, focused on overcoming resistant hypertension, using steroidal and nonsteroidal MRAs to reduce cardiorenal risk, determining which patients are good candidates for newer SGLT2 and GLP-1 agents, and insights on the continuum of heart failure.
Opening Remarks
Before Dr. Ferdinand delivered his opening remarks, attendees completed a pretest to gauge their familiarity with the day's topics
Keith C. Ferdinand, MD, cardiologist at Tulane University School of Medicine, enjoyed a heartfelt introduction which included a nod to his Living Legends Award from the Southern University at New Orleans Center for African and African American Studies. As he took the stage he acknowledged the disproportionate health effects of COVID-19 and attributed them in large part to social determinants of health. “Social determinants are the main driver of these big disparities. There are some genetics involved but I don’t think they can explain these huge gaps in morbidity and mortality.” One of the social determinants Dr. Ferdinand mentioned were ‘food swamps,’ or the tendency for the local store or bodega in low-income neighborhoods to be full of highly processed foods and sugar-sweetened beverages. “This affects the health and well-being of our patients that live in these communities, which in turn affects our ability as clinicians to really make a difference,” said Dr. Ferdinand.
Dr. Ferdinand introduces the speakers and topics for the final day of education at the 18th Annual CMHC
Tackling the Disproportionate Burden of Resistant Hypertension in Black Adults: Perspectives and Advances
The disproportionate degree to which racial and ethnic populations, especially African Americans, shoulder the burden of hypertension is driven mainly by social determinants of health. “How can we overcome the mortality gap? This is not social science. I’m not talking about a bad Tweet or Facebook post. I’m talking about mortality,” said Dr. Ferdinand to open his lecture on tackling hypertension disparities.
"Undertreatment and therapeutic inertia are the primary causes of resistant hypertension. Some strategies to overcome this are using team-based care to deliver standardized treatment protocols and empowering the patient to control their blood pressure using self-monitoring technologies."
Resistant Hypertension: Definitions, Current Treatment and Emerging Approaches
Dr. Ferdinand invited Debbie L. Cohen, MD, to the stage for a session on new and emerging drugs and devices to address treatment-resistant hypertension (TRH). She first defined TRH as “A patient whose blood pressure is above the target of 130/80 mmHg with concurrent use of three antihypertensive medications at maximally tolerated doses, including a diuretic.” She then described some new devices for renal denervation, saying “There is a real role for this procedure in certain patients with hypertension that hasn’t responded to pharmacotherapy.” She referenced the SPYRAL-HTN OFF MED trial from 2020 that investigated changes in systolic and diastolic blood pressure measured over a 24-hour ambulatory period for three months after renal denervation with Medtronic’s Spyral catheter.
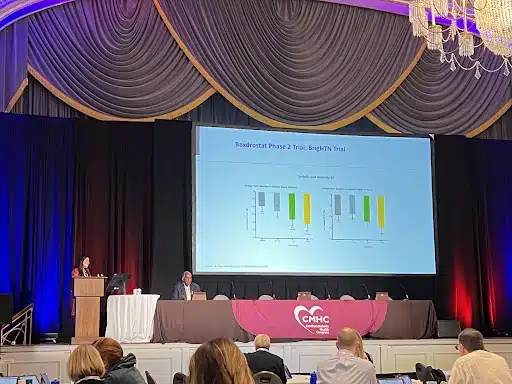
Dr. Cohen presents exciting new data on baxdrostat, a selective aldosterone synthase inhibitor showing promise for resistant hypertension
"Please check your patients with resistant hypertension for primary aldosteronism. It is present in at least 20 to 30% of your patients who aren't responding to their drugs."
Sleep and Hypertension: A Two-Way Street
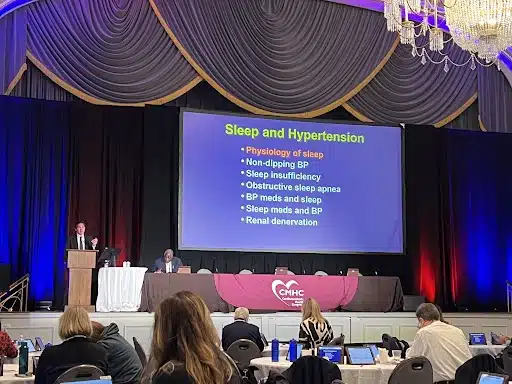
Sleep expert Dr. Somers outlines the topics he'll discuss during his lecture on the complex relationship between sleep and blood pressure
Virend K. Somers, MD, PhD, took the stage to lend his perspectives on the reciprocal relationship between disordered sleep and the development or worsening of hypertension. He dispelled some misconceptions about the use of melatonin supplements, saying “Melatonin is meant to regulate sleep cycles, not induce sleep.” The natural way to induce the body’s melatonin production is to induce darkness in the four hours preceding bedtime and avoid electronics in the bedroom. He got a laugh from the audience when he stressed that the bedroom is for “Sleep and sex, only,” highlighting the detrimental effects of watching TV, working on your laptop, or doing other activities in bed that contribute to poor sleep hygiene and may lead to cardiometabolic consequences.
"Just because sleep apnea and hypertension are happening in the same patient doesn't mean that the apnea is causing the high blood pressure. If patient begins using a CPAP to treat sleep apnea you can't assume it will also treat their hypertension."
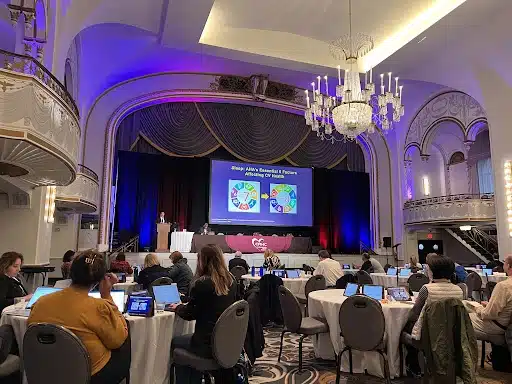
Dr. Somers explains the addition of a sleep metric to the American Heart Association's checklist for heart health, Life's Essential 8™
The Role of Steroidal and Nonsteroidal MRAs in Cardiorenal Risk Reduction
Next up, Ajay K. Singh, MBBS, FRCP, MBA, introduced the concept of cardiorenal medicine by saying “The heart and the kidneys tango together.” He explained that the inflammation in diabetes contributes to fibrosis and glomerulosclerosis, which ultimately leads to diabetic kidney disease, kidney failure and heart failure. “You need to treat cardiorenal patients in multiple ways. When you think about the hemodynamics you see in both the kidney and the heart, think about inflammation and fibrosis because these factors conspire to make cardiorenal syndrome so difficult to treat,” said Dr. Singh.
"Treating patients with spironolactone does reduce systemic blood pressure and glomerular pressure, but the primary effects are thought to be in fibrosis. That's why this therapy is so interesting, because you have multiple ways to try and target the cardiorenal syndrome."
Dr. Singh overviews the three types of cardiorenal syndrome
Which Patients Should Get SGLT2s and GLP-1s for Cardiorenal Risk Reduction?
"You've heard about many available agents to treat heart failure, but there's a lot to consider when making prescribing decisions. Cost, polypharmacy and adherence are challenges above and beyond just the functionality of any given drug."
Challenging Cardiorenal Cases and Expert Panel Discussion
The final day of the conference culminated with all six of the faculty presenters returning to the stage to discuss some of their trickiest patient cases. Dr. Taub began with a case of a 73-year old woman she was interested in beginning on an SGLT2 inhibitor. “We are talking about improving outcomes instead of improving symptoms, which is an improvement even over the conversations we were having a few years ago,” commented Dr. Somers when addressing Dr. Taub’s patient with asymptomatic heart failure.
Next, Dr. Cohen introduced the audience to her case of a 33-year old male patient with poorly controlled severe hypertension. “I’m just imagining this patient in my advanced heart failure clinic in five years, so I would be super aggressive about getting him on a therapeutic regimen now because his heart is working way too hard,” Dr. Morris weighed in.
“If they wake up in the morning with weakness or vision issues, particularly in patients with type 2 diabetes, that indicates their blood pressure isn’t dipping enough during sleep,” contributed Dr. Somers, drawing on his expertise in sleep science regarding Dr. Cohen’s patient case.
From L to R: Drs. Ferdinand, Morris, Somers, Cohen and Singh discuss a patient case presented by Dr. Taub (not pictured)
Thank you, Boston!
That’s a wrap! Thank you to the faculty, staff, exhibitors, and most of all our audience of multidisciplinary providers who seek out strategies rooted in evidence to provide informed care to their patients!
Although we have concluded another successful CMHC event at the Boston Park Plaza, it’s never too early to start planning your attendance at next year’s conference! Register for the 19th Annual CMHC now and use special code Annual24 to instantly save $200 on the registration fee. The coupon code expires on 10/31/23.